


INTRODUCTION
Essential thrombocythemia (ET) is a chronic myeloproliferative disorder characterized by platelet overproduction. Despite being a rare disease, its incidence increases with age, with most patients presenting between the ages of 50 and 60 years, although this can also be observed in young patients. It is more common in females, as reported in 65% of 1,494 patients with ET [1]. Thrombosis is the most common cause of mortality and morbidity in patients with ET. Few reports have described an increased risk of bleeding associated with ET. Extreme ET (platelet count of >1,500,000 mcL, i.e., >1,500,000×109/L) may increase the risk of bleeding [2]. Currently, there are no universally agreed clinical guidelines for the perioperative management of patients with ET. Herein, a patient with ET who underwent operative gynecologic laparoscopy developed unpredictable postoperative prolonged intraperitoneal bleeding.
CASE REPORT
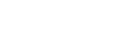
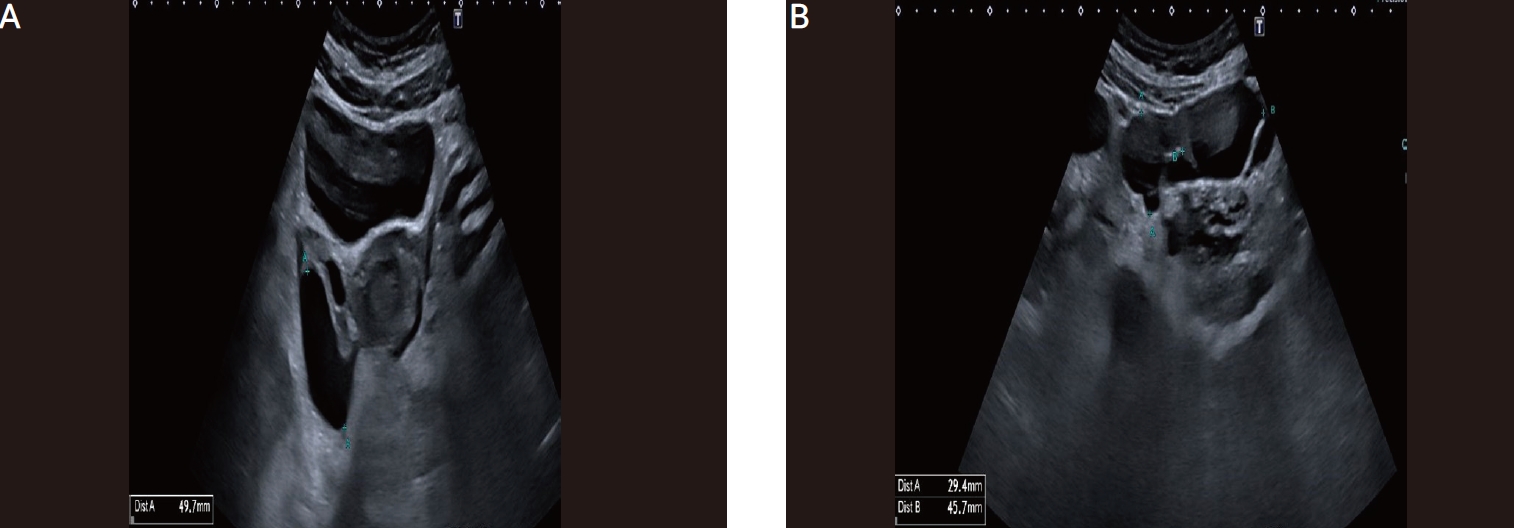
A 32-year-old patient who had been married for 7 months presented to the outpatient department (OPD) complaining of chronic pelvic pain and dyspareunia. Clinically, bilateral pelvic tenderness increased as the cervix was moved. Transvaginal ultrasonography (Fig. 1) and magnetic resonance imaging (Fig. 2) revealed a left adnexal cystic mass suggestive of a large hydrosalpinx adhering to the back of the uterus with possible extensive pelvic adhesions. She had a history of bone marrow biopsy that revealed ET and was administered cytotoxic treatment (500-mg hydroxyurea in two capsules, taken orally daily for 8 years). Preoperative complete blood count (CBC) showed thrombocytosis (597,000 mcL), whereas other routine laboratory test results, including hemoglobin level (13 g) and coagulation profile, were normal. The treating hematologist was consulted and cleared her for laparoscopy, which was approved by anesthesiologists. Diagnostic laparoscopy revealed a large hydrosalpinx on the left side (Fig. 3); a distally occluded right tube (small hydrosalpinx); and extensive adhesions to the colon, omentum, and back of the uterus. Adhesiolysis, a right salpingoneostomy with refashioning of a new ostium using the thermal flowering technique, followed by left salpingectomy of the completely pathologic left fallopian tube, was performed. After ensuring a normal blood pressure, a negative suction drain was inserted to ensure meticulous hemostasis. The early postoperative period was relatively short. The suction drain was filled with 20 mL of serosanguinous fluid. Once the patients started ambulation approximately 4 hours postoperatively, the suction drain started to collect a significant amount of pure blood, reaching 350 mL. Supportive treatment was administered in the form of parenteral IV fluids, tranexamic acid, and ethamsylate ampoules but failed to stop the trickling of blood. Her vital signs were stable; however, drain trickling persisted. After consultation with hematologists, blood transfusion was performed. Abdominal ultrasonography revealed no significant intraperitoneal collections in the hepatorenal pouch or behind the uterus. The patient was vitally stable after blood transfusion, supportive treatment, and administration of parenteral fluids. After 15 hours of persistent blood trickling, a decision to perform a second-look rescue laparoscopy was made to search for the source. It revealed a mild, insignificant ooze at the trocar site and a mesosalpingeal site that were meticulously coagulated. No active bleeding of blood vessels was observed. The entire peritoneum was highly congested and bled easily in the minimal pouch. Small areas of peritoneal petechiae were scattered away from the surgical site. No intraperitoneal irrigation fluid or blood clots were observed. At the end of the laparoscopy, hemostasis was securely checked with normal blood pressure. However, the suction drain continued to ooze over the following 6 hours, which required consultation with the general surgery team, who decided on a longitudinal abdominal exploration of the whole abdomen after correction of the general condition of the patient, which started to deteriorate due to continuous trickling. Their decision was based on revision of the second laparoscopy video and their fear that the patient might have had a hidden upper abdominal injury during abdominal entry. Again, exploration revealed insignificant surgical findings to explain the continuous oozing of blood, apart from the congested peritoneum. On the second day, computed tomography angiography was performed to identify the source of bleeding; however, the results were normal. The decision was made to repeat the replacement of oozing blood with frequent CBC testing in the S-ICU. The platelet count was fluctuating between 740,000 and 952,000 mcL. Within 5 days, the blood oozing declined gradually, and the drain became serosanguinous until complete cessation on day 7. She was then transferred to the regular care ward of the OB/GYN department for 2 days before being discharged from the hospital. She received eight units of fresh blood and 14 units of fresh frozen plasma, in addition to some units of thrombocyte concentrate and cryoprecipitate. After discharge, she was followed up in the OPD and was well without significant complaints. The patient signed a consent form to publish her case.
DISCUSSION
According to the World Health Organization (WHO), ET is diagnosed based on four major criteria, or the first three major criteria and one minor criterion. First three major criteria include a platelet count of ≥ 450×109; bone marrow biopsy showing proliferation (mainly of the megakaryocyte lineage, with increased numbers of enlarged, mature megakaryocytes that have hyper-lobulated nuclei; no significant increase or left shift in neutrophil granulopoiesis or erythropoiesis; and extremely rarely a minor grade 1 increase in reticulin fibers); and not meeting the WHO criteria for BCR-ABL1-positive CML, PV, PMF, myelodysplastic syndromes, or other myeloid neoplasms. The fourth major criterion is the presence of JAK2, CALR, and MPL mutations. Minor criteria include the presence of a clonal marker or absence of evidence of reactive thrombocytosis [3]. It can cause thrombosis but can also cause bleeding, neurological abnormalities, and even obstructive ileus [4,5]. It seems strange that one disease can paradoxically lead to thrombosis and bleeding tendencies, contributing to most of the associated morbidities and mortalities. Currently, there are clinical guidelines for the perioperative management of patients with ET. Further studies are required to provide clear guidelines for both medical and surgical interventions aimed at preventing thrombo-hemorrhagic complications associated with ET.
Bleeding is associated with extreme ET that may lead to acquired von Willebrand syndrome. In this case report, postoperative bleeding was noted even though the preoperative platelet count did not reach extremely high levels, and the patient was cleared by hematologists. This event may warn against the liberal clearance of patients with ET based solely on the platelet count. Therefore, additional safety assessment parameters should be used to clarify these cases. Some studies [6] have tested flow cytometry as a promising method for platelet function testing because it is independent of platelet count. Therefore, flow cytometry can be used in patients with altered platelet counts, making it suitable for testing platelet function [7]. Others evaluated platelet function in ET under different analytical conditions using light-transmission aggregometry in platelet-rich plasma (PRP) and impedance aggregometry in PRP and whole blood and found defective platelet functions under the least physiological conditions in cases of ET [8]. There is an urgent need for a quick and easy test for platelet function in patients with ET. If a platelet function test had been performed for this case report, the patient would have been saved from additional surgeries to identify the cause of the abnormal bleeding. Because the patient in this case report had used hydroxyurea for 8 years, there is a great need for a detailed study of the effect of cytotoxic drugs on bleeding tendency in patients with ET. Hydroxyurea can lead to a significant reduction in the number of blood cells [9], which was not observed in the present study. Others performed laparoscopic surgery while the patients were receiving anagrelide [10]. In conclusion, patients with ET should consent to rare but possible post-laparoscopic bleeding. Surgeons should offer these treatments to ensure hemostasis. A preoperative study of platelet function and the selection of the best cytotoxic medication for the perioperative period are required.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






