Safety of radiotherapy in patients with Behcet’s disease: a case report and review of the literature
Article information
Abstract
Exaggerated acute and late toxicities following radiotherapy have been reported in patients with pre-existing connective tissue diseases, such as systemic lupus and scleroderma. Behcet’s disease (BD) is a relapsing multisystem connective tissue disease characterized by vasculitis in the mucocutaneous, ocular, gastrointestinal, respiratory, neurologic, urogenital, articular, and cardiovascular systems. Data concerning the relationship between radiotherapy toxicity and BD are limited in the literature. Here, we report a case of lung cancer treated with radiotherapy (60 Gy) in a patient with BD. No severe radiation-induced toxicity was observed. Radiation-induced toxicity in patients with BD has also been discussed.
INTRODUCTION
Behcet’s disease (BD) is a relapsing inflammatory disorder of unknown etiology that manifests as recurrent oral aphthous ulcers, genital ulcers, uveitis, and skin lesions [1]. Most reports on severe toxicities, such as skin atrophy, skin necrosis, and fibrosis, after radiotherapy in patients with connective tissue diseases, involve patients with systemic lupus, rheumatoid arthritis, or scleroderma [2]. However, data concerning the relationship between radiotherapy toxicity and BD are limited in the literature. Herein, we describe the case of a patient with concomitant lung cancer and BD. Radiation- induced toxicity in patients with BD has also been discussed.
CASE REPORT
In February 2018, a 70-year-old man presented with a 3.5-cm nodule in the left upper lobe of the lung on chest radiography. The patient was a 50 pack-year current smoker with a medical history of hypertension, atrial fibrillation, intracerebral hemorrhage, and left middle cerebral artery infarction. The patient quit smoking in May 2018. Twenty-three years prior to presenting with the lung nodule, the patient underwent clipping surgery for a cerebral artery aneurysm. At that time, he was diagnosed with BD, with symptoms of recurrent oral and genital ulcers, and knee arthritis and was prescribed oral colchicine. In addition to the chest X-ray, a computed tomographic scan of the chest revealed a 3.8-cm malignant-looking mass in the left perihilar area and an enlarged lymph node in the left hilum. Surgery was recommended, but the patient refused.
In March 2019, the patient presented with dyspnea on exertion, cough, a 10-kg weight loss over the previous year, general weakness, and loss of appetite. The Eastern Cooperative Oncology Group performance status score was 2. Bronchoscopy revealed total obstruction of the left upper lobe main bronchus with a mass. Biopsy of the primary tumor revealed a poorly differentiated squamous cell carcinoma. Computed tomography of the chest revealed obstructive atelectasis and necrotizing pneumonia in the left upper lobe, enlarged lymph nodes in the left paratracheal area, hilum, and subcarina, and left malignant pleural effusion. Irregular atherosclerotic wall thickening in the aortic arch and abdominal aorta, penetrating ulcers at the aortic arch, and aneurysmal dilatation in the ascending aorta (4.3 cm) and descending thoracic aorta (3.5 cm) were also noted. The clinical stage was T4 N2 M1a. The patient had been treated with oral colchicine for BD at the time of radiotherapy. Oral and genital ulcers had been stable for 9 months before radiotherapy. Palliative radiotherapy for left upper lobe obstruction was recommended. The primary left hilar lesion received 60 Gy in 30 fractions (Figs. 1, 2). During radiotherapy, the patient experienced grade 1 esophagitis and a grade 1 skin reaction (redness on the anterior chest wall and back) (Table 1). One month after completion of radiotherapy, the primary left hilar lesion had decreased and the obstruction of the left upper lobe main bronchus had improved; however, lumbar spine (L1) metastasis and single 7-mm brain metastasis in the right medial temporal lobe developed. Hippocampus- sparing whole brain radiotherapy with simultaneous integrated boost was applied at 35 Gy in 10 fractions for the right medial temporal lobe gross tumor and at 25 Gy in 10 fractions for the whole brain. The lumbar spine received 30 Gy in 10 fractions. No radiation-induced toxicities were observed. The patient did not undergo chemotherapy. In August 2019, 6 weeks after the completion of spine and brain radiotherapy, the patient died from obstructive pneumonia in the left upper lobe. This study was approved by the Institutional Review Board of the Jeju National University Hospital (IRB No. 2021-03-07).
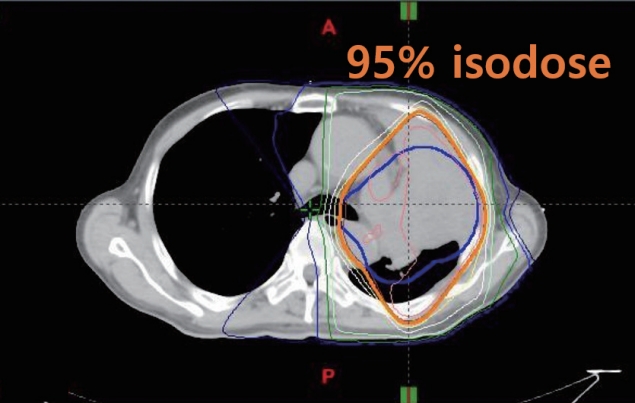
Isodose curves on an axial image.

Dose volume histogram curves.

Toxicity related to radiotherapy in our case
DISCUSSION
In our case, there was no severe acute or late radiation-induced toxicity in the lung or mediastinum. Karatas et al. [3] reported no radiation-induced toxicity in 10 patients with breast cancer. Na et al. [4] reported that radiotherapy was performed in three patients (breast, rectum, and colon) without complications (Table 2). On the other hand, several severe acute and late radiation-induced toxicity events have been reported in patients with BD [2,5,6]. Chargari et al. [5] observed grade 3 epithelitis during adjuvant radiotherapy (44 Gy in 22 fractions) in a patient with breast cancer, which resulted in an interruption of radiotherapy. Meyer et al. [2] reported a bronchoesophageal fistula 5 weeks after the completion of definitive radiotherapy (64 Gy) and chemotherapy (cisplatin and etoposide) in a patient with lung cancer. They recommended considering screening for esophageal ulcers before initiating treatment for thoracic tumors in patients with BD.2) Concurrent use of chemotherapy and high radiation dose may have contributed to the severe toxicity. Cengiz et al. [6] reported three severe late toxicity reactions after radiotherapy in patients with BD (Table 2). A patient with Hodgkin’s disease developed brachial plexopathy (pain in the left upper arm) 6 months after the completion of radiotherapy (40 Gy) to the mantle field. Another patient developed left ureteral stricture 4 months after the completion of postoperative radiotherapy (50 Gy) for cervical cancer. A third patient with a thigh mesenchymal tumor developed skin necrosis 6 months after the completion of postoperative radiotherapy (70 Gy).
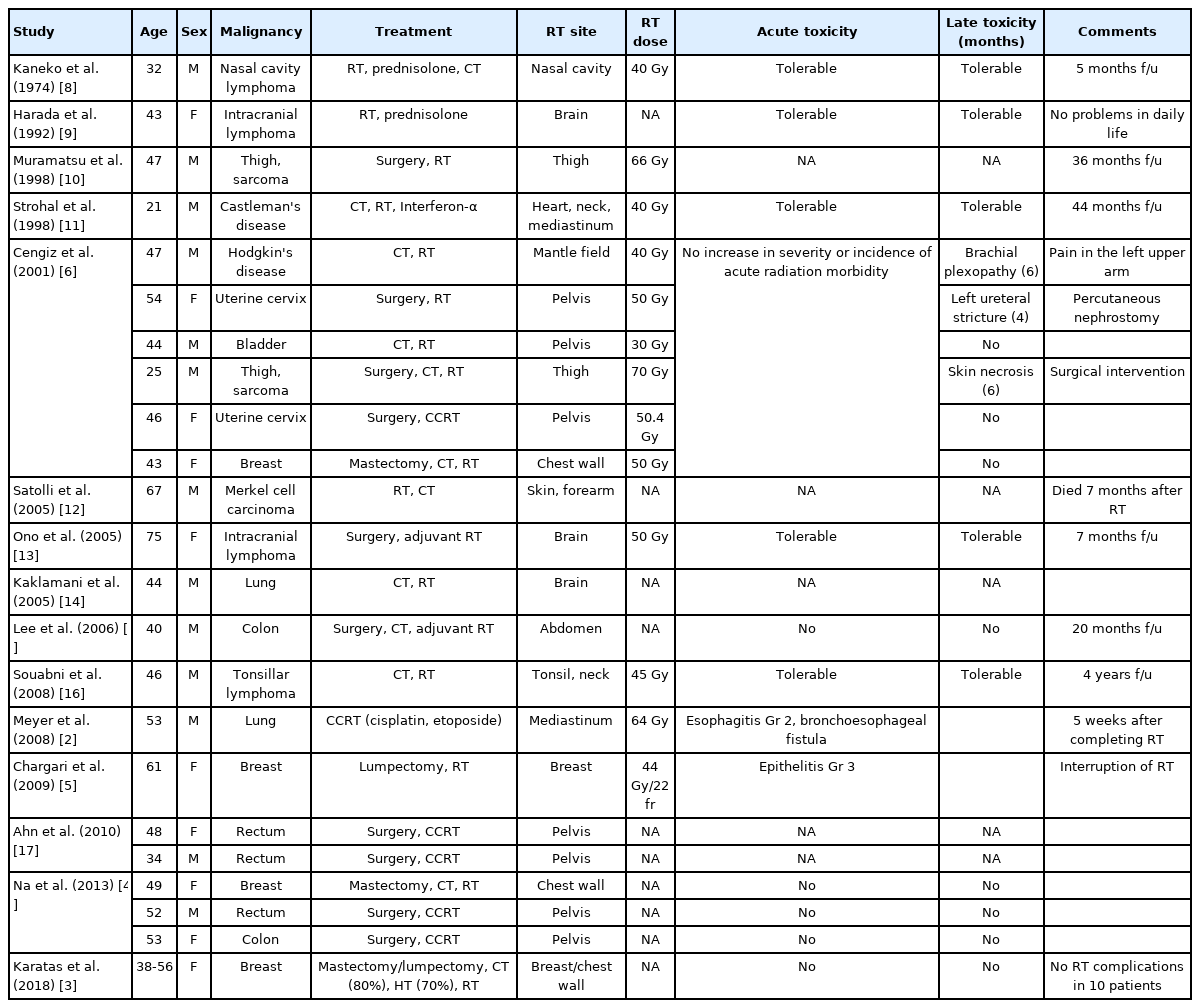
Toxicity related to radiotherapy in cancer patients with Behcet’s disease
The pathogenesis of BD remains unclear. A combination of infectious agents, immune disorders, environmental factors, and genetic factors may be related to BD [7]. Benderli Cihan et al. [7] recommended that during periods of exacerbation, BD patients receiving radiation treatment should be closely monitored for acute and chronic toxicity. In our case, recurrent oral and genital ulcers had been quiescent for 9 months before radiotherapy.
CONCLUSIONS
A limitation of our report is that the follow-up period after the completion of radiotherapy was only 4 months, which is too short to evaluate the effects of late toxicity. The total radiation dose and treatment volume can affect the level of toxicity. In our case, the total radiation dose was 60 Gy, and most of the esophagus and mediastinum were excluded from the scope of the radiation treatment. These factors may have contributed to mild toxicity.
The relationship between BD and radiation-induced toxicity remains controversial. Several severe acute and late radiation- induced toxicity events have been reported. We need to be cautious when applying radiotherapy in patients with BD. Further studies regarding acute and late toxicity may be required to clarify the safety of radiotherapy in patients with BD.