Auricular conchal cartilage for treatment of empty nose syndrome
Article information

Abstract
Empty nose syndrome is an uncommon complication of turbinoplasty and other nasal operations. It presents with various manifestations, with the most common symptom being paradoxical nasal obstruction. Here, we report the case of a 67-year-old male patient diagnosed with empty nose syndrome 20 years after turbinoplasty. Autologous auricular conchal cartilage was harvested and implanted into the lateral wall of the inferior turbinate to reduce nasal volume. The patient experienced significant relief from subjective nasal obstruction symptoms immediately after surgery. Over a 23-month follow-up period, no side effects or symptom recurrence was reported.
INTRODUCTION
Empty nose syndrome (ENS) is a term coined by Eugene Kern in 1994 and is recognized as a form of secondary atrophic rhinitis that rarely occurs after nasal surgery but is typically iatrogenic [1]. Increased nasal cavity volume and changes to nasal airflow can lead to atrophy of the nasal mucosa. This leads to paradoxical symptoms, such as nasal obstruction, dryness, bad odor, pain, and epistaxis [1]. Treatment for this syndrome may include non-surgical options like nasal irrigation and topical ointments. If these therapies do not yield improvement, surgical intervention may be necessary to reduce the nasal cavity’s volume [2].
In this report, we describe a case of ENS that was successfully resolved using autologous auricular cartilage grafting. The patient was suspected of developing the condition after excessive turbinoplasty. We present this case report along with a review of the existing literature.
CASE REPORT
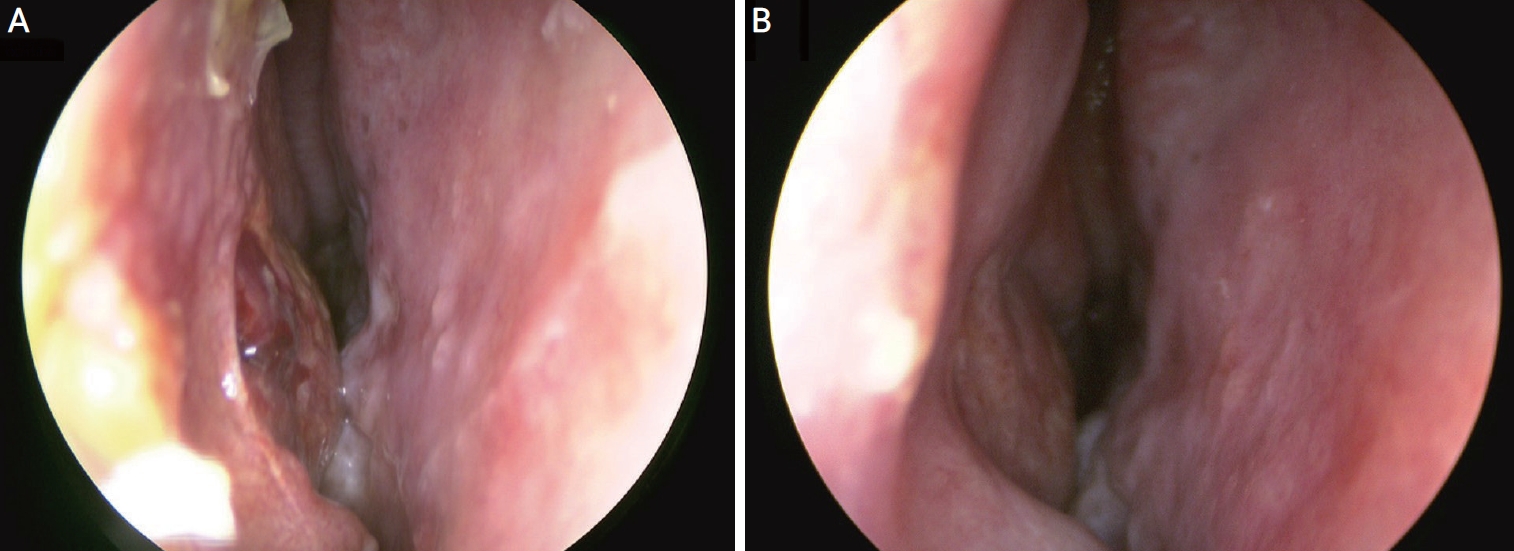
A 67-year-old male patient visited our hospital, reporting persistent right nasal congestion over several years. The patient mentioned previous treatments at a private clinic, including the application of local steroid ointments and nasal irrigation, which provided temporary symptom relief. Nasal endoscopy revealed dryness and atrophy of the nasal mucosa, with partial defects in the anterior regions of both inferior turbinates (Fig. 1). The patient expressed a desire to rip off his nose, specifically complaining about severe nighttime congestion that hindered sleep. The patient scored 18 on the nasal obstructive symptom evaluation (NOSE) scale and 9 on the visual analogue scale (VAS) for nasal obstruction. This study was approved by the Institutional Review Board (IRB) of Chungbuk National University Hospital (IRB No. 2022-10-010). Getting informed consent was waived from the IRB.

Preoperative endoscopic findings. (A) Right nasal cavity, (B) left nasal cavity.
The patient had a history of nasal septal deviation and snoring, for which he underwent septoplasty and turbinoplasty in a private hospital 20 years ago. Computed tomography (CT) revealed excessive resection of both inferior turbinates but no evidence of mucosal thickening or septal deviation (Fig. 2). A cotton test was utilized to further support the diagnosis of ENS, where the inferior turbinate area was temporarily expanded with a cotton ball before surgery, resulting in immediate symptom relief (Fig. 3).
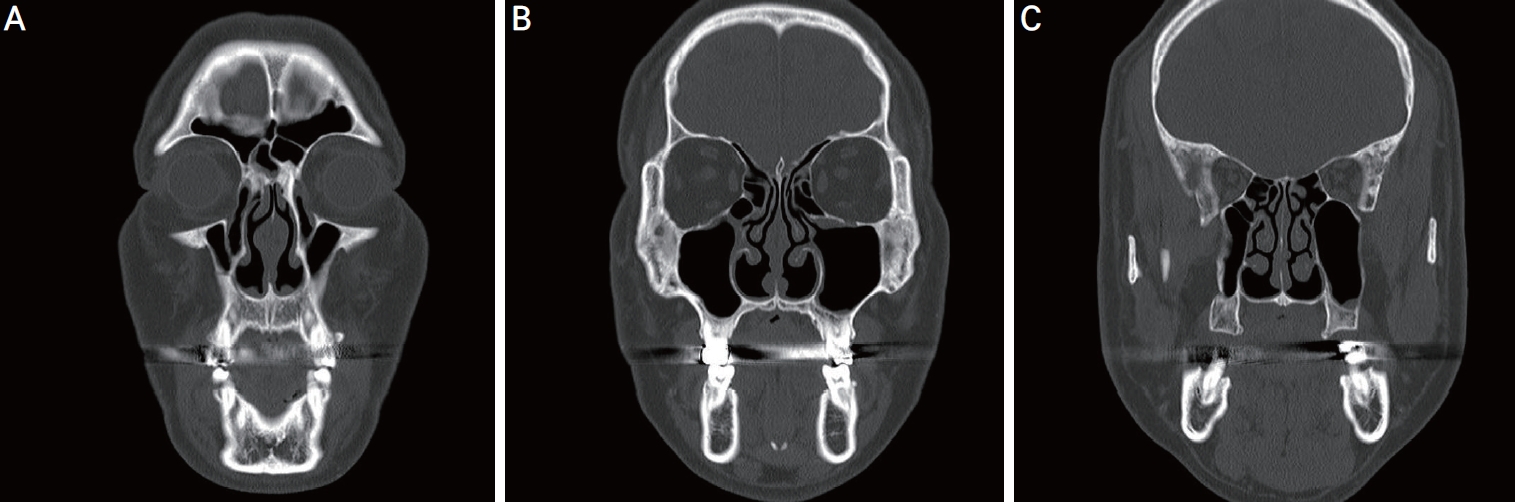
(A-C) Preoperative facial bone CT findings (coronal view). CT: computed tomography.

Endoscopic image of a cotton test. After cotton was placed into the narrow right inferior meatus, nasal obstruction symptoms improved immediately.
After a thorough discussion with the patient, surgery harvesting auricular cartilage from the right ear to reduce the volume of the right nasal cavity was performed. Under general anesthesia, an incision was made on the front of the right ear to obtain cartilage. The skin and perichondrium were dissected, and a crescent-shaped incision was made to isolate the cartilage from the perichondrium. After infiltrating the right inferior turbinate wall with a 2% lidocaine solution containing 1:100,000 epinephrine, the mucosa was evaluated using a Freer elevator. A trimmed cartilage piece was inserted into the mucosa, and the elevated mucosa was repositioned, completing the procedure with absorbable sutures (Fig. 4).
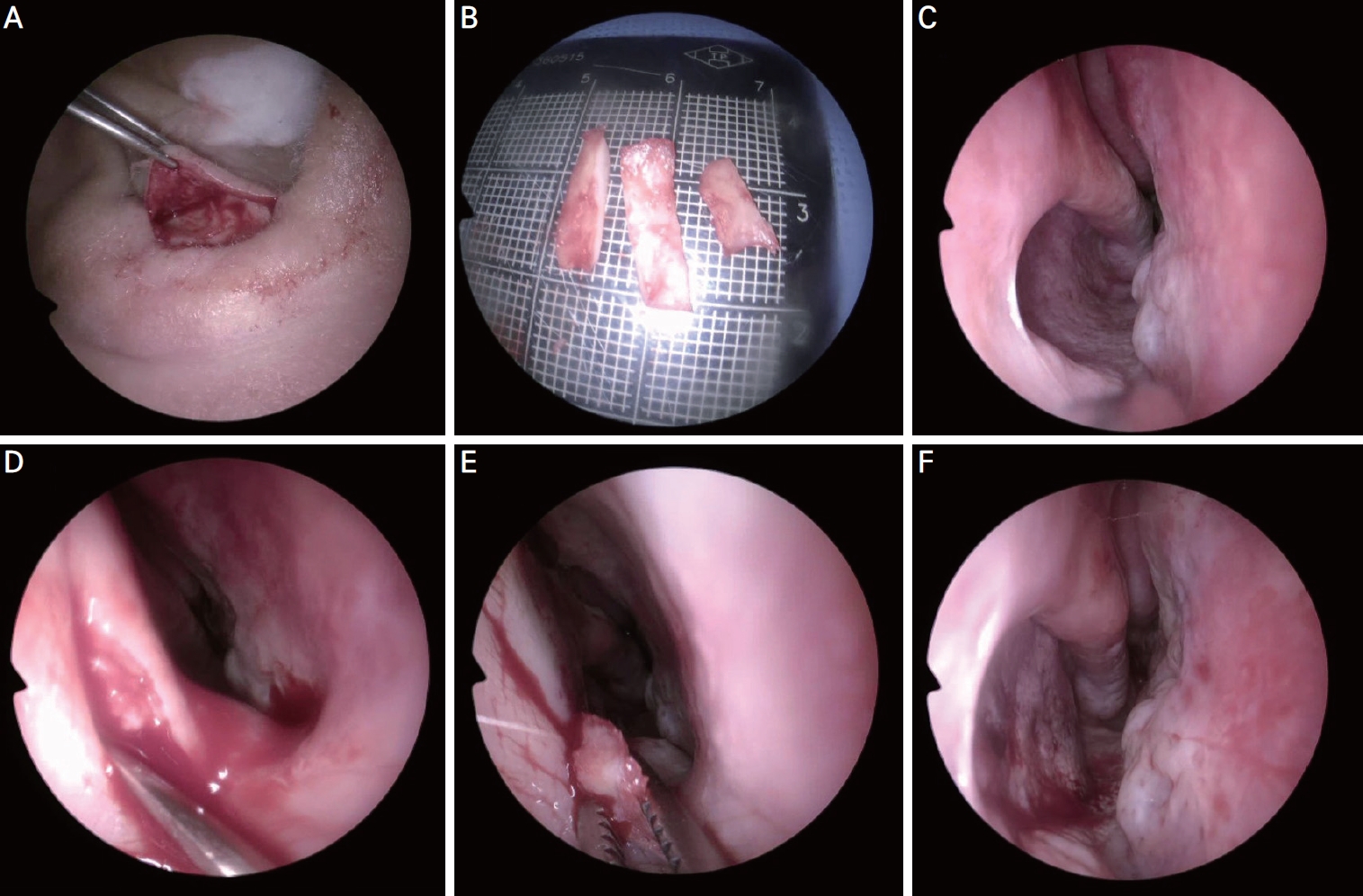
Operation procedures for empty nose syndrome. (A) Harvesting auricular conchal cartilage. (B) The harvested auricular cartilage was sliced into three pieces before implantation into the inferior meatus. (C) Endoscopic view of the right nasal cavity before the operation. (D) An incision was made anterior to the right inferior turbinate. Dissection was performed using Freer’s elevator to create space for cartilage implantation. (E) The sliced cartilage pieces were implanted into the created space on the right lateral wall. (F) The right inferior meatus was narrowed by inserting auricular cartilage.
The patient experienced immediate symptom improvement after the surgery, expressing satisfaction and relief. During the 6-month follow-up, the patient scored 5 points on the NOSE scale and 1 point on the nasal obstruction VAS scale. There was no recurrence of previously discomforting symptoms. Nasal endoscopy confirmed a decrease in volume of the right inferior turbinate wall compared to before surgery, as additional cartilage was used to reduce the nasal cavity volume (Fig. 5). Twenty-three months post-surgery, the patient did not report any discomfort or symptoms.
Postoperative endoscopic findings of the right nasal cavity. Postoperative (A) 1 week, (B) 1 month.
DISCUSSION
ENS is a condition characterized by mucosal atrophy in the nasal cavity. Although its exact causes remain poorly understood, it occurs when the nasal cavity becomes excessively wide for various reasons, leading to decreased airflow resistance and sensory impairment of airflow [3]. The incidence of ENS is approximately 20% of patients who undergo turbinoplasty [4]. Since there is no specific diagnostic criteria, understanding the patient’s subjective symptoms and medical history is crucial. It is also necessary to confirm the absence of nasal structures through nasal endoscopy and CT scans. The cotton test, using a cotton ball to examine symptom improvement, can be valuable for both diagnosis and predicting surgical outcomes [5]. In this case, the cotton test was performed before surgery and clearly demonstrated improvement, further supporting the diagnosis of ENS.
First-line treatment for ENS typically involves maintaining nasal cavity humidity through measures such as nasal irrigation, local steroids, and topical ointments. If symptoms persist despite these treatments, surgical intervention may be considered. In this patient’s case, despite attempts at nasal irrigation and topical ointment application, symptoms remained severe to the point of causing suicidal ideation. This prompted the decision to proceed with surgical treatment after a thorough discussion and consideration of any adverse outcomes. While there was an observation of increased nasal cavities on both sides due to the excessive resection of both inferior turbinates, the patient clearly complained of nasal obstruction only on the right side. After a thorough consultation with the patient, surgery was performed only on the right side.
Surgical intervention aims to reduce nasal cavity volume, promote the regeneration of normal mucosa, and enhance the lubricating ability of dry nasal mucosa. The ideal approach is to transplant turbinate cartilage into deficient inferior turbinate tissue. However, if insufficient turbinate tissue is available for transplantation, the nasal septum, lateral wall, or floor of the nasal cavity could be alternative sites [6]. Various graft materials can be used for this procedure, including acellular dermis, silicone plates, and autologous grafts such as septal or auricular cartilage, and bone [7,8]. In this case, auricular cartilage was used as graft material because the patient had a history of septal surgery, which made it challenging to obtain sufficient septal cartilage. Auricular cartilage is commonly used and easily accessible for ENT surgery, with advantages such as ease of manipulation, resistance to infection, and relatively minimal volume loss due to absorption, unlike other autologous graft materials [9]. Some clinicians have also introduced filler injections as a graft material [10]. Injecting fillers under the mucosa of the anterior nasal septum can narrow the nasal valve area, resulting in favorable effects. However, filler volume is reduced from 6 to 12 months after injection. In the case of worsening symptoms, additional filler injections or long-term filler maintenance may be necessary.
ENS primarily occurs as a secondary complication after nasal surgery and is challenging to treat. Therefore, prevention is essential when performing initial surgeries related to nasal diseases. Specifically during turbinoplasty, it is crucial to preserve at least half the volume of the inferior turbinate. Even when performing submucosal resections using a microdebrider, preserving as much mucosa as possible is recommended [5].
Favorable results were achieved in the surgical treatment of ENS that developed after nasal surgery, using autologous auricular conchal cartilage transplantation. This method is a possible surgical option for managing ENS.