Spontaneous resolution of new coronary artery aneurysm following guideline-directed medical therapy after drug-eluting stent implantation
Article information

Abstract
Here, we present a case of a 56-year-old man with acute myocardial infarction. The patient underwent percutaneous coronary intervention (PCI) at the left main bifurcation and mid-left anterior descending artery using drugeluting stents. Four months after the PCI, the patient was readmitted for cardiac arrest. Coronary angiography (CAG) revealed stent thrombosis in the left main-toproximal left anterior descending artery and in-stent restenosis in the left main-toproximal left circumflex artery. We performed balloon angioplasty at the left main to mid-left anterior descending artery and left main to proximal left circumflex artery stents; subsequently, blood flow was fully restored. However, contrast agent extravasation was observed outside the mid-portion of the left main artery to the proximal left anterior descending artery stent, indicating the presence of a coronary artery aneurysm (CAA) outside the stent. After guideline-directed medical therapy with dual antiplatelet agents and high-intensity statins, follow-up CAG revealed near-resolution of the CAA, absence of stenotic lesions, and good blood flow.
INTRODUCTION
A coronary artery aneurysm (CAA) was first described in 1812 by Bougon, who found a ruptured right coronary artery (RCA) at the post-mortem of a patient who died suddenly [1]. A CAA is defined as a regional coronary artery dilatation greater than 1.5 times the normal adjacent segment diameter [2]. The incidence of CAA is very rare, ranging from 0.3% to 5.3%, with pooled data showing a mean incidence rate of 1.65% [3]. Atherosclerosis is the most common cause of coronary artery aneurysm. Other possible causes of CAAs include inflammation, infections, vasculitis, connective tissue diseases, and trauma [4,5]. Complications include embolization, thrombosis, and ischemia [6,7]. There are no management protocols for CAA. Here, we describe a case in which CAA that occurred after percutaneous coronary intervention (PCI) with drug-eluting stents (DES) spontaneously resolved after optimal medical therapy.
CASE REPORT
A 56-year-old male presented at our hospital with chest pain. His coronary artery disease risk factors included smoking and diabetes mellitus. He was taking the following medications for diabetes mellitus and dyslipidemia: metformin 1,000 mg, alogliptin 25 mg, and atorvastatin 10 mg. His blood pressure was 113/75 mmHg, and laboratory test results were as follows: low-density lipoprotein cholesterol (LDL-C), 82 mg/dL; glycated hemoglobin (HbA1c), 6.4%; and C-reactive protein (CRP), 0.93 mg/dL. Electrocardiography showed ST-segment elevation myocardial infarction, and emergent coronary angiography (CAG) was performed. CAG showed near total occlusion with severely calcified lesions at the left main (LM) bifurcation (Fig. 1A), mid left anterior descending artery (mLAD), and distal RCA. A 7 Fr sheath was inserted through the right femoral artery and the coronary artery was engaged using a 7 Fr Judkins left four guiding catheters. A 0.014-inch Sion wire and 0.014-inch Sion blue wire were inserted into the left anterior descending artery (LAD) and left circumflex artery (LCX), respectively. Balloon angioplasty (BA) was performed to dilate the LM to the mLAD and the LM to the proximal LCX (pLCX) using a 2.5×15 mm balloon. After predilation, additional BA was performed with 3.0×15 mm non-compliant (NC) balloon. Two stents (Resolute Onyx 3.0×38 mm at the mLAD; Resolute Onyx 3.5×38 mm at the LM to the proximal LAD [pLAD]; Medtronic, Minneapolis, MN, USA) were deployed, and another stent (Resolute Onyx 4.0×18 mm; Medtronic) was inflated at the LM to the pLCX using the culotte technique. Kissing ballooning was then performed using a 3.5×22 mm stent balloon (Medtronic) at the LM to the pLAD and a 4.0×15 mm NC balloon (Medtronic) at the LM to the pLCX. The final angiogram (Fig. 1B) and intravascular ultrasonography (Fig. 1C) revealed no stenotic lesions and good blood flow.

(A) Coronary angiogram shows stenosis with severe calcification in the LM bifurcation. (B) Coronary angiogram immediately after drug-eluting stent implantation to LM bifurcation. (C) Intravascular ultrasound at the site of the arrow in (B) indicating the stent distal edge showed good expansion and apposition of the stent. LM: left main.
Four months after the initial PCI, the patient was readmitted because of chest pain and cardiac arrest. At the time, he was on the following medications: aspirin, ticagrelor, atorvastatin, carvedilol, metformin, and dapagliflozin. His blood pressure was 109/67 mmHg, and laboratory test results were as follows: LDL-C, 69 mg/dL, HbA1c, 6.7%, and CRP, 0.17 mg/dL. CAG revealed ST from the LM to pLAD and in-stent restenosis (ISR) from the LM to pLCX (Fig. 2A). We performed BA at the LM to the mLAD and LM to the pLCX stents, and the blood flow fully recovered (Fig. 2B). However, the contrast agent was observed collecting outside of the mid portion of LM to pLAD stent, indicating that the CAA (8.3×7.6 mm2) had occurred outside of the stent on CAG (Fig. 2C) and coronary computed tomography angiography (Fig. 2D). After BA for the ST and ISR lesions, the patient was administered high-intensity statin therapy, specifically rosuvastatin 20 mg, while continuing dual antiplatelet agents consisting of aspirin and prasugrel.
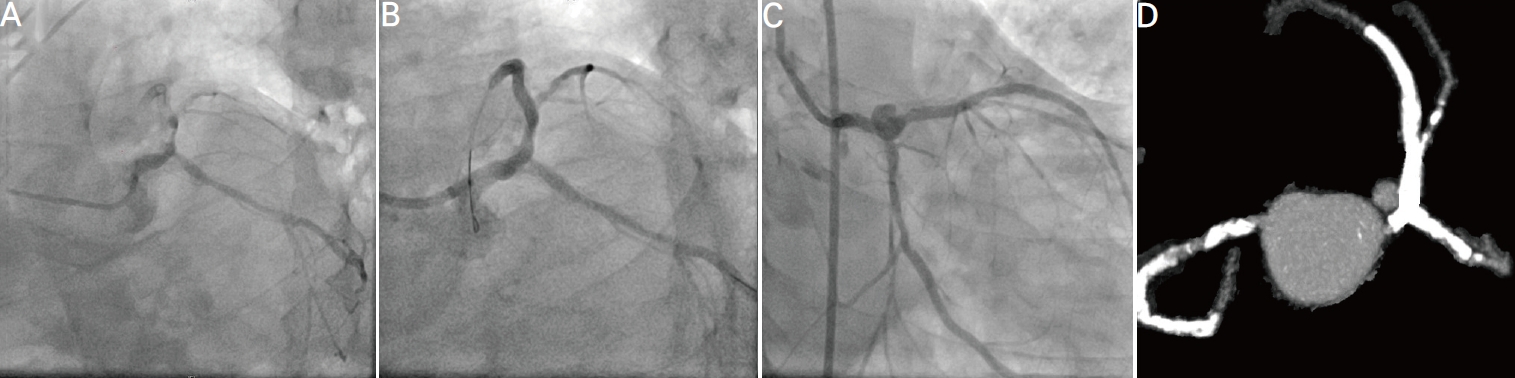
(A) Four months after the initial percutaneous coronary intervention, stent thrombosis in LM to proximal left descending artery stent and in-stent restenosis in LM to proximal left circumflex artery stent on coronary angiogram. (B) Coronary angiogram after drug-eluting balloon angioplasty at LM bifurcation. (C) The new coronary aneurysm (8.3×7.6 mm2) in mid portion of the LM-proximal left anterior descending artery stent was shown on coronary angiogram and (D) coronary computed tomography angiography. LM: left main.
At 12 months after initial PCI, the patient’s current medication includes ezetimibe, which was added compared to before. His blood pressure was 116/78 mmHg, and laboratory test results were as follows: LDL-C, 22 mg/dL; HbA1c, 6.7%; CRP, 0.40 mg/dL. Follow-up CAG revealed a near-resolution CAA, absence of stenotic lesions, and good blood flow (Fig. 3).
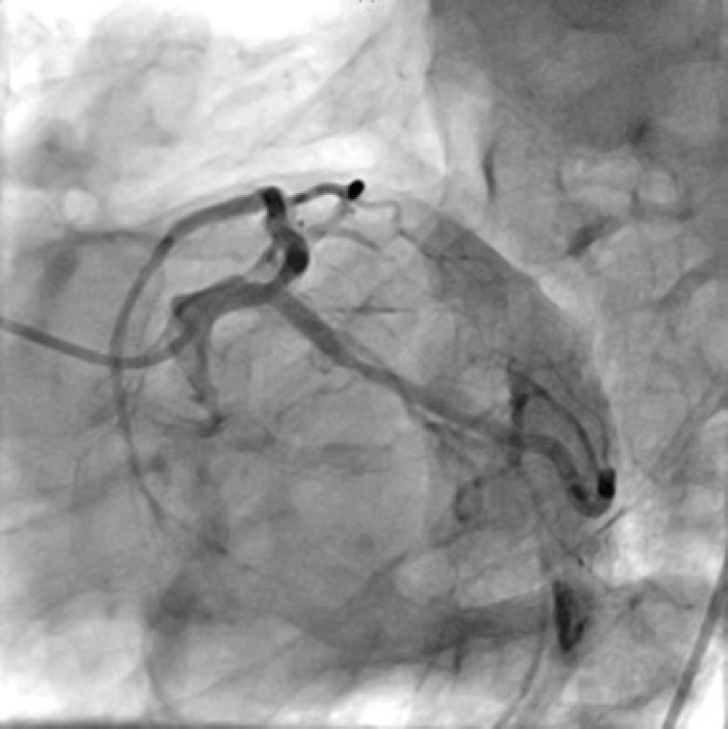
Twelve-month follow-up coronary angiogram shows near complete, spontaneous resolution of the aneurysm and no significant stenosis of coronary artery.
DISCUSSION
We describe a case of spontaneous resolution of a coronary artery aneurysm approximately 1 year after PCI with a DES. The patient was diagnosed with a new coronary aneurysm formation after DES implantation using CAG and coronary computed tomography. The occurrence of new coronary aneurysms after stent implantation poses a risk of ST and ISR. Although the incidence of new CAA complicating DES is known to be very low, concerns have been raised regarding the outcomes of new coronary aneurysms after DES implantation due to the substantial morbidity related to CAA [8]. The formation of new CAA is more commonly observed because of residual dissection and deep arterial wall injury caused by oversized balloons or stents and high-pressure balloon inflation. DES may lead to late complications in the coronary arterial wall, including aneurysm formation, stent thrombosis, incomplete stent apposition, and vessel rupture. Possible mechanisms, including local hypersensitivity vasculitis in response to polymers or coating drugs, have been postulated [4,9], but the exact cause and pathophysiology remain unknown. The natural history of DES-related aneurysms is not well defined. In most cases, conservative management is pursued. However, conservative management carries potential complications such as thrombosis, rupture, and sudden death. Therefore, management of these complications remains controversial. Recently, several reports have suggested that implantation of covered stents into CAA could be a viable solution for this lesion. Surgery with ligation of the CAA is an alternative treatment for high-risk patients [10]. However, appropriate therapeutic strategies for DES-related aneurysms are not well established.
In conclusion, this was an extremely rare case of new CAA formation, occurring 3 months after DES deployment, with delayed healing over the next year.
Acknowledgements
The authors declare no conflicts of interest in this article.