무릎전치환술 환자에서 일회성 복재신경차단술이 수술 후 출혈량 감소에 미치는 영향
A single injection of saphenous nerve block reduces postoperative bleeding after total knee arthroplasty
Article information
Trans Abstract
In elderly patients, the vital parameters tend to fluctuate based on the blood volume status, which may cause sudden hypovolemic shock if the postoperative bleeding continues. Particularly, those who undergo surgery for arthritis needs to pay extra attention because the bleeding may persist over the joints after the surgery. Therefore, appropriate pain control is required to reduce the postoperative blood loss. This retrospective chart review study was conducted to assess the postoperative pain control and reduction of blood loss with a single injection of saphenous nerve block (SNB) in elderly patients with osteoarthritis. We reviewed the electronic medical records of patients who underwent knee total arthroplasty with spinal anesthesia between January and May 2016. A total of 51 patients participated in this study. All patients were treated with intravenous patient-controlled analgesia for the postoperative pain control, and additional analgesic agents were administered at a visual analogue scale above a score of 6. In 25 patients, SNB was performed using ultrasound with the administration of 0.75% ropivacaine (15 mL) after the surgery. Patients who received additional analgesics were significantly low in the nerve block group (P=0.009). Additionally, the volume of blood loss from catheter drainage was significantly low at 2 and 3 days postoperatively (P=0.013 and P=0.041, respectively) in the nerve block group. In patients who underwent total knee arthroplasty with osteoarthritis, only a single injection of saphenous nerve block was sufficient for the postoperative pain control and reduced bleeding.
서론
수술 후 통증은 무릎관절치환술 후 환자들이 호소하는 심한 불편감 중 하나로, 관절 부위 회복을 위하여 물리 치료 및 관절가동을 진행하는 데 중요한 방해요인으로 작용한다. 조기 보행과 물리치료는 회복을 빠르게 하고, 혈전색전증이나 감염과 같은 수술 후 발생 가능한 합병증의 위험을 감소시키는 것으로 알려져 있기 때문에 수술 후 적절한 통증 조절이 중요하다. 또한 관절 수술 후에도 일정 기간 수술 부위의 출혈이 지속되므로 적절한 통증 조절은 술 후 출혈량을 감소시키는 데에도 영향을 미치는 것으로 알려져 있다[1]. 이러한 제통작용과 출혈량과의 관계는 통증 조절을 위해 사용하는 마약성 진통제의 투여가 히스타민 분비로 이어져 말초혈관 확장을 유발하여 출혈량 증가시킨다거나 통증으로 인한 교감신경 자극이 동맥혈압 상승을 유발하여 출혈량을 증가시키는 것으로 알려져 있다[2]. 이때 통증 조절을 위하여 흔히 사용하는 방법으로 정맥용 주사약제를 사용하거나 그 외에도 경막외 카테터를 거치하여 약물을 투여하는 방법, 신경차단술을 이용하는 방법 등이 대표적이다[2-4].
본 연구에서는 척추마취 하에 무릎전치환술을 받은 환자에서 적절한 통증 조절이 수술 후 출혈량 감소와 연관될 것이라는 가설 하에 수술 후 통증 조절을 위하여 기존의 정맥용 자가통증조절장치를 사용하는 방법과 비교하여 일회성 복재신경차단술을 함께 시행한 환자에서 통증 조절 및 수술 후 출혈량 감소에 미치는 영향을 알아보고자 한다.
대상 및 방법
본 연구는 제주대학교병원 연구윤리위원회의 인증을 받아 진행되었다(IRB No. 2020-04-004).
1. 연구 대상
2016년 1월부터 2016년 5월까지 제주대학교병원에서 척추마취 하에 편측 무릎전치환술을 받은 환자 중 미국마취과학회 신체등급분류 1-3의 환자를 대상으로 총 51명의 환자가 등록되었다. 마취의에 따라 마취 및 수술 후 관리에 사용하는 약물의 프로토콜이 다를 수 있으므로 이러한 bias를 피하기 위하여 특정 마취의가 해당 환자들을 마취한 기간 동안을 연구 기간에 포함시키기 위하여 일정 기간을 한정하였다. 제외 대상은 심각한 심장질환이나 심박차단, 관상동맥질환이 있는 환자, 신기능 및 간기능 저하가 동반된 환자, 정신지체 환자, 술 전 저혈압 혹은 저혈량증이 동반된 환자, 수술 후 부득이하게 배액 카테터가 제거된 환자, 자가통증조절장치 사용을 거부한 환자, 동측 수술 후 재수술을 시행하는 환자, 의무기록차트 내의 자료가 누락된 환자 등이다.
2. 연구 방법
의무기록을 확인하여 대상 환자를 선별한 뒤 의무기록지를 활용하여 해당 데이터를 수집하고 환자의 개인정보를 삭제한 후 엑셀로 저장하였다. 자료 수집은 정해진 프로토콜에 따라 환자 그룹을 알지 못하는 1인이 동일한 기록지를 리뷰하여 엑셀로 정리된 사항을 추후 환자군으로 정리하여 통계 분석을 시행하였다. 기본 의무기록지에서 환자의 나이, 성별, 키, 몸무게, body mass index, 과거력 등에 대한 정보를 얻고 마취기록지에서는 신경차단 시행 여부, 총 마취시간, 총 수술시간에 대한 데이터를 저장하였다. 간호기록지에서 술 후 마약성 약물의 투여 후 발생한 구역, 구토, 어지럼증과 같은 부작용 여부와 추가 진통제 투여 여부를 확인하고 배액관을 통해 측정된 출혈량을 하루 단위로 합산하여 해당 데이터를 저장하였다. 이 때 통증 조절 정도를 알아보기 위하여 수술 후 병동에서 추가 약물 투여 횟수를 비교하였고, 출혈량 감소를 알아보기 위하여 수술 후 배액 카테터를 통한 출혈량을 비교하여 분석하였다. 환자군은 아래와 같이 수술 중 추가로 복재신경차단술을 시행하였는지 여부에 따라 두 군으로 분류하였다: 1) intravenous (IV)군: 수술 후 통증 조절을 위하여 정맥용 자가통증조절법을 사용한 환자군, 2) saphenous nerve block (SNB)군: 수술 후 통증 조절을 위하여 정맥주사제를 이용한 자가통증조절법을 사용하고 추가로 수술 종료 시점에서 일회성 복재신경차단술을 초음파 검사(Philips Ultrasound Inc., Bothell, WA, USA) 하에 신경 주변에 0.75% ropivacaine 15 mL를 주입한 환자군.
모든 환자는 수술 후 통증 조절을 위하여 정맥용 자가통증조절장치를 사용하였다. 통증척도(visual analogue scale, VAS) 6점 이상인 경우 통증 조절이 불충분하다고 판단하여 병동에서 주치의의 오더에 따라 추가적인 약물(tramadol 50 mg 또는 pethidine 25 mg)이 투여되었다. 추가 약물 투여 여부는 수술 후 3일째까지의 의무기록을 바탕으로 하였으며, 자가통증조절장치와 함께 추가 투여된 마약성 진통제에 의한 구역, 구토, 어지럼증 등의 부작용 여부를 확인하였다. 수술 후 수혈의 기준은 혈중 혈색소 수치가 9 mg/dL 미만이거나 혈액검사 당시에는 9 mg/dL 이상 11 mg/dL 미만이라 하더라도 빈맥, 저혈압, 어지럼증과 같이 증상이 동반되고 일반 수액제제 만으로 증상 회복이 어려운 경우에는 수혈을 진행하였다. 일반적으로 환자들은 수술 후 1일째 지속적인 수동운동(continuous passive motion)을 시작하여 수술 후 3일째 자가통증조절장치와 수술 부위의 배액 카테터를 제거하면서 워커를 이용한 보행운동을 진행하였다.
3. 통계 분석
정맥주사용 자가통증조절장치를 단독으로 사용한 군과 복재신경차단술을 추가로 시행한 군의 두 군을 분석 비교하였다. 모든 분석은 SPSS (version 18.0; IBM Corp., New York, NY, USA)를 이용하였다. 결과는 연속변수인 경우 평균값±표준편차로, 양적변수인 경우 퍼센트로 나타냈다. 이전 연구에 따르면 수술 후 48시간 동안 opioid 사용량이 13.5±7.5 mg으로 type I (α) 에러 0.05, type II (β) 에러 0.20, 표준편차 7.8로 10% 배제된다는 가정 하에 샘플 사이즈는 28명이다[5]. 그러나 앞서 언급한 것처럼 일정 기간 동안 기준에 맞는 환자들을 포함시켜 진행하여 제외된 환자수가 많았다. 평균치 비교가 필요할 경우에는 T-test를 시행하였고 비연속변수는 Pearson’s chi-square test, Fisher’s exact test로 검정하였다. 반복측정변수에 대해서는 repeated measured analysis of variance를 사용하여 검정하였고, P<0.05이면 통계적으로 유의하다고 판정하였다.
결과
해당 기간 동안 총 81명의 연구 대상자 중 재수술 4건, 양측수술 22건, 자가통증조절장치 거부 4건으로 30명의 환자가 제외되어 대상 환자는 51명이었고 그중 IV군과 SNB군은 각각 26명, 25명이었다(Fig. 1). 환자들은 평균 70세 이상 연령층으로 두 군 간 인구학적 통계나 수술시간 및 마취시간에는 유의한 차이가 없었다(Table 1).

CONSORT flow diagram. IV group: administration of patient-controlled analgesia intravenously, SNB group: administration of patient-controlled analgesia intravenously and a single shot of SNB. PCA: patient-controlled analgesia, IV: intravenous, SNB: saphenous nerve block, CONSORT: Consolidated Standards of Reporting Trials.
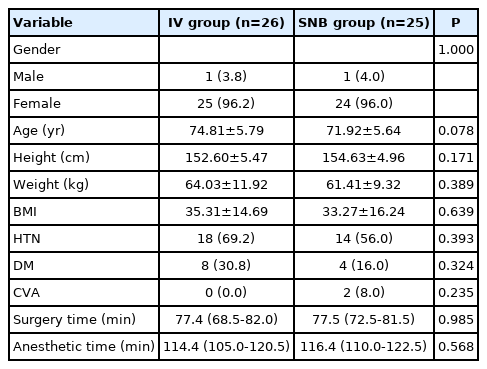
Demographic and perioperative data
수술 후 환자관리에서 진통제 투여에 의한 부작용으로 구역, 구토, 어지럼증 등이 발생한 환자는 IV군에서 더 많았지만 통계적 유의한 차이를 나타내지는 않았다(Table 2). 그러나 VAS 6 이상으로 자가통증조절장치 이외의 추가 진통제가 투여된 환자는 IV군에서 24명인 반면에 SNB군은 15명으로 통계적으로 유의하게 IV군에서 더 많았다(P=0.009).
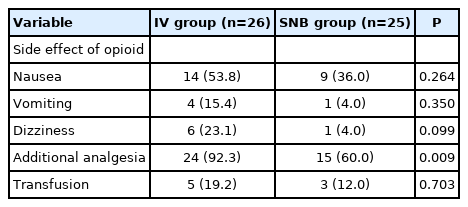
Management of patients in postoperative period
두 군 간 수술 후 출혈량은 수술을 시행한 당일과 수술 후 1일째에는 유의한 차이를 보이지 않았으나 수술 후 2일째, 3일째에는 IV군에 비하여 SNB군에서 각각 70.0 mL (95% 신뢰구간, 10.57-83.35; P=0.013)와 22.80 mL (95% 신뢰구간, 1.30-48.94; P=0.041)로 통계적으로 유의하게 적은 양이 배액되었다(Fig. 2). 그러나 수술 당일부터 수술 후 3일째까지 출혈량 감소 추이에서는 두 군 간 큰 차이를 보이지 않았다(P=0.162).
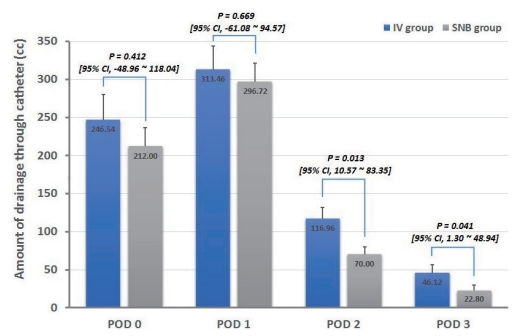
Graph comparing the amount of blood drained through the catheter at the surgical site after surgery by date. Error bars indicate the standard error of mean. P value and confidence interval were evaluated using Student’s t-test. IV group: administration of patient-controlled analgesia intravenously, SNB group: administration of patient-controlled analgesia intravenously and a single shot of saphenous nerve block. POD: postoperative day, CI: confidence interval, IV: intravenous, SNB: saphenous nerve block.
고찰
본 연구는 일회성 복재신경차단술로 수술 후 통증 경감 효과에 대한 유용성에 초점을 맞춘 이전 발표된 연구들에 비하여 통증 완화와 함께 궁극적으로 수술 후 출혈량 감소에 미치는 영향을 확인하기 위한 연구로, 자가통증조절장치만 사용한 군에 비하여 수술 종료 시점에서 일회성 신경차단술을 추가로 시행한 군에서 통증 경감 효과와 수술 부위에서 배액된 출혈량이 유의하게 감소하여 수술 후 환자관리에 유용하게 시행해 볼 수 있다는 결과를 도출하였다.
무릎관절 수술에서 통증 조절을 목적으로 시행하는 신경차단술 중 고식적으로 사용되던 방법은 대퇴신경차단술이다. 지속적 대퇴신경차단술에서 환자의 움직임에 따라 카테터 관리가 어려운 반면 일회성 신경차단주사 후 혈관주사만 유지하기 때문에 환자의 움직임이나 이동에 주의를 요하지 않아 관리가 더욱 원활하여 술 후 환자의 안전을 위하여 도움이 될 수 있다[2,4,6]. 또한 대퇴신경차단술은 대퇴네갈래근의 강도가 약화되어 낙상의 위험이 있는 것으로 알려져 있다. 반면에 복재신경차단술은 근육의 강도에 큰 영향을 미치지 않아 오히려 효과적이라는 연구들이 진행된 바 있다[7-9]. 그러므로 시술에 의한 부작용 없이 적절한 통증 조절을 위한 여러 가지 연구들이 현재까지도 진행되고 있는 추세이다.
통증 조절 정도는 VAS와 같은 통증지표를 비교하는 것이 일반적이나, 본 연구에서는 일정 시간 간격으로 프로토콜화된 지침에 따라 측정한 것이 아니었으므로 차트 기록만으로 결과값이 차이를 유발할 수 있다. 따라서 저자들은 추가 진통제의 투여 여부를 통증 조절 결과지표로 사용하였다. 그 결과 SNB군에서 추가 진통제 투여가 유의하게 적었는데, 이는 수술 종료 때 시행한 신경차단술의 효과가 수술 후 초기 진통 작용에 IV군에 비하여 효과적으로 작용한 것으로 볼 수 있다.
또한 적절한 통증 조절은 출혈량 감소에 영향을 미친다는 연구들이 보고된 바 있다[2,10]. 비록 수혈 진행이 두 군 간 유의한 차이가 없었다 하더라도(P=0.703, Table 2) 혈색소(hemoglobin), 적혈구용적률(hematocrit) 수치는 수혈 후 증가할 수 있기 때문에 출혈량을 측정하는 데 객관적 지표로 작용하지 못할 우려가 있다. 따라서 본 연구에서는 실제 수술 부위에서 배액된 양을 출혈량 지표로 두 군 간의 차이를 비교하였다. Figure 1에서 보여지듯 수술 당일과 수술 후 1일째에는 물론 IV군에서 평균 출혈량 자체는 더 많았으나 통계적으로 유의한 차이를 보이지 않았다. 그러나 수술 후 2일째와 3일째에서는 SNB군에서 확연히 출혈량이 감소한 것을 확인할 수 있었다. 관절 수술을 받는 환자들은 고령의 환자들이 많아서 기저질환이 많고 체액량 변화에 민감하여 세심한 주의가 필요하다. 따라서 이러한 결과는 술 후 수혈 빈도를 감소시키고 환자의 체액량을 유지하여 환자를 안전하게 관리하는 데 도움을 준다.
본 연구는 단일기관에서 한 명의 마취의에 의해서 시행된 시술에 대한 결과로 상대적으로 대상 환자수가 많지 않으며, 본원에서 슬관절치환술을 받는 환자에서 여성의 비율이 높아 대부분의 환자들이 여성이었다는 제한점이 있다. 또한 후향적 연구로 진행되어 결과에 바이어스로 영향을 미칠 수 있는 요소들을 배제하기 어렵기 때문에 유용하게 활용 가능한 지표들을 사용하는 데에도 한계가 있었다. 의무기록지를 바탕으로 결과값들을 리뷰하는 과정에서 선후관계가 불분명하거나 동일한 시간대에 누락된 값들로 다양한 결과를 얻는 데에 어려움이 있었던 것은 본 연구의 큰 제한점이다.
물론 통계적으로 유의한 결과가 임상적으로도 의미가 있다고 정의하기는 어렵다. 본 연구의 결과에서 배액 카테터를 통한 출혈량 감소를 확인하였다고 하더라도 실제 수혈 시행 횟수 감소나 재활 기간 동안 운동량의 월등한 우월성을 입증하지는 못하였다. 그럼에도 불구하고 수술 후 초기의 심한 통증을 경감시키려 적극적으로 관리하는 것은 노인환자들의 예후에 도움이 됨과 동시에 환자의 편의와 안전을 위하여 임상에서 지속적으로 노력해야 하는 부분이다[11,12].
저자들은 본 연구를 통하여 슬관절전치환술을 받은 환자에서 시행한 일회성 복재신경차단술은 특별한 부작용 없이 수술 후 통증 조절에 도움이 될 뿐만 아니라 이와 같은 적절한 통증 조절로 인해 수술 후 출혈량 감소에 도움을 줄 수 있음을 확인하였다.